BLOOD VISCOSITY FUNCTIONAL PARAMETERS
BIOMECHANICS OF VEHICLE IMPACT
FINGERPRINT AS A BIOMETRIC IDENTITY
TISSUE ENGINEERING: A MULTIDISCIPLINARY FIELD OF BIOMEDICAL ENGINEERING
BLOOD VISCOSITY FUNCTIONAL PARAMETERS
-Bipin Upadhyay
The friction forces that act within a moving fluid are termed as viscosity. In more specified way viscosity can be defined from the figure below. A fluid is located between two parallel plates. The shear force, F, divided by the contact area between the liquid and the plate gives the shear stress, (τ).
.jpg)
The shear rate is the difference in velocity between the different layers and can here be calculated as the velocity of the top plate (the bottom plate does not move) and the distance between the plates, i.e., shear rate is γ = v/h. The ratio of shear stress and shear rate is the viscosity. If we change the plate velocity or change the distance between the plates, shear stress and shear rate will change. The slope of the relation between shear stress-shear rates gives the viscosity (η).
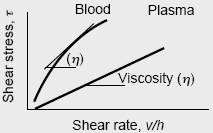
If a straight line is obtained, as for plasma, we call the fluid Newtonian. Newtonian fluid, η is independent of shear rate (but can depend upon such parameters as temperature, and liquid or gas composition). Many fluids, however, possess the characteristic that η changes as the shear rate changes and are therefore termed “non-Newtonian” fluids. From above figure, Shear stress is directly proportional to shear rate for Newtonian fluid only.
The main function of the circulating blood is to carry oxygen and other nutrients through the body and to remove carbon dioxide and waste products. However, blood also transports other substances, such as hormones, white blood cells, and platelets, to sites within the body where they are needed. Thus, blood is also important for hemostasis (the prevention of blood loss when the vascular system is damaged) as well as immune defense. Blood is a suspension of red blood cells (erythrocytes), white blood cells (leukocytes) and platelets in a complex solution (called plasma) of gases, salts, proteins, carbohydrates, and lipids. The viscosity, or internal friction, of blood increases as the percentage of cells in the blood increases: more cells mean more friction, which means a greater viscosity.
The percentage of the volume of a blood sample occupied by cells, is determined by a centrifuge or device which separates the cells and other particulate elements of the blood from the plasma. The remaining fraction of the blood sample is called plasmocrit (blood plasma volume) and the percentage of the blood volume occupied by red blood cells is called the hematocrit. If blood is allowed to clot, the remaining fluid is called serum, which is similar to plasma, but is missing the fibrinogen. Red blood cells number about 5 ×106 per mm3. They are disk-shaped, measuring about 7.6 μm in diameter and 2.8 μm in thickness. With a normal hematocrit of about 40 (that is, approximately 40% of the blood volume is red blood cells and the remainder plasma), the viscosity of whole blood (cells plus plasma) is about 3 times that of water. On the other hand, the viscosity of plasma alone is about 1.5 times that of water.
Although the concentrations and types of proteins in the plasma can affect its viscosity, this has little, if any, effect on the overall viscosity of whole blood. When the hematocrit rises to 60 or 70, which it often does in patients with polycythemia, or abnormally high red blood cell counts, the blood viscosity can become as high as 10 times that of water. Alternatively, when the hematocrit falls drastically, as it does in patients with anemia (a decreased number of red cells in the blood), blood viscosity can approach that of plasma alone. The coefficient of viscosity for water is 0.001 Newton-second per meter squared (N-s/m2) at 20 degrees Celsius. The coefficient of viscosity for whole blood at 37 degrees Celsius, and at a physiological hematocrit of 45 is 0.0027 N-s/m2.
.jpg)
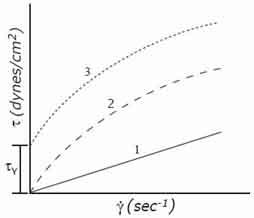
Flow curve of simple type of fluid
A plot of shear stress, τ, versus shear rate is called a flow curve. Examples are shown in figure above. Curve 1 is for a Newtonian fluid in which viscosity is independent of shear rate. The slope of the curve is the coefficient of viscosity; η. Curve 2 shows a behavior seen in solutions of high polymers in which the viscosity is a function of shear rate. In the curve shown, the viscosity decreases with increasing shear rates (a “shear-thinning” fluid). The fluid shown in curve 3 behaves as a solid at low levels of shear stress, but begins to flow when some critical “yield stress”, τy , is exceeded. If the curve were linear for τ>τy , the material would be known as a “Bingham plastic”. It is a “shear-thinning” curve of the type shown in curve 2 of figure shown above.
The viscosity of blood thus depends on the viscosity of the plasma, in combination with the hematocrit (Ht). Higher hematocrit implies higher viscosity. The relation between hematocrit and viscosity is complex and many formulas exist. One of the simplest is the one by Einstein:
η = η plasma (1 + 2.5 Ht)
Viscosity is function of hematocrit
Blood behaves very differently in our circulatory system than water flowing in pipes. First of all, blood has a higher viscosity (thickness) than water. Increased blood viscosity causes the blood flow to be pulsatile and the flow rate varies with time. The reason for the pulsatile flow is two-fold, a resultant of the ejection portion of the cardiac cycle and because the arterial wall is elastic. The arterial system is not a straight pipe; it has many bifurcations and bends. Pulsatile blood flow imparts energy into the arterial system that the protective adaptation process theory organizes the arterial system’s adaptative process into two cycles, both of which originate from the mechanical stresses in the system.
The viscosity of blood depends on its velocity of the blood. More exactly formulated, when velocity (shear rate) increases viscosity decreases. At higher velocity the disc-shaped Red Blood cells (RBC’s, erythrocytes) orient in the direction of the flow and viscosity is lower. For extremely low shear rates formation of RBC aggregates may occur, thereby increasing viscosity to very high values. It has even been suggested that a certain minimum shear stress is required before the blood will start to flow, the so-called yield stress. In large and medium size arteries shear rates are higher than 100 1/s, so viscosity is practically constant. The physiological range of wall shear stress is 10 to 20 dynes/cm2.
In 1931 Fahraeus and Lindqvist measured the viscosity of blood, relative to that of water, in thin glass tubes at high shear rates. They observed a decrease in relative viscosity when tube diameter fell below 0.3 mm. The explanation of this effect is the fact that RBCs tend to migrate toward the center of the tube, leaving a cell-poor layer of plasma (of lower viscosity) near the walls. It is also true that the effective hematocrit in a thin tube is lower than that in a reservoir feeding the tube. (The RBCs at the center of the tube move faster than the plasma at the walls; thus, to transport the same ratio of cells to plasma through the tube, the concentration of RBCs must be lower than at the feeding reservoir.)
.jpg)
.jpg)
The viscosity depends on the size of blood vessel (Fahraeus-Lindqvist effect). In small blood vessels, and at higher velocities, blood viscosity apparently decreases with decreasing vessel size. This effect begins to play a role in vessels smaller than 1 mm in diameter.
The anomalous character of blood viscosity results from the red blood cells, and the effects are mainly found in the microcirculation at low shear and small diameters. The effects are of little importance for the haemodynamics of the larger arteries. Thus in haemodynamics it may be assumed that viscosity is independent of vessel size and shear rate.
Viscosity as the function of shear rate
Viscosity as function of vessel size
for hematocrit of 48
Viscosity is strongly dependent on temperature. A decrease of 1°C in temperature yields a 2% increase in viscosity. Thus in a cold foot blood viscosity is much higher than in the brain.
From all of the above, we may conclude that to a good approximation. Blood may be considered as a Newtonian fluid only if the radius of the vessel exceeds 0.3 mm and if the shear rate exceeds 100 sec-1. This condition, therefore, excludes arterioles, venules, and capillaries. The viscosity of blood is a strong function of the hematocrit.
References:
- Gehrhart, P.M., and Gross, R.J. Fundamentals of Fluid Mechanics. Addison-Wesley, Reading, Mass. 1985.
- http://www.vilastic.com/tech10.html
- http://www.virgina.edu/rjh9u/blood.html
- Kamm, Prof. Roger. Physiological Fluid Mechanics. Harvard-MIT Division of Health Sciences and Technology.
- Fung, Y.C., Bio mechanics Circulation, Second Edition, Springer, 2004.
BIOMECHANICS OF VEHICLE IMPACT
-Ram Chandra Poudel, BE
Faculty Member, Mechanical Engineering
Biomechanics deals with formal and quantitative analysis of relationships between structures and functions of living tissues and the application of the results to man in health and disease. As such, biomechanics is an area common to mechanics, matter, physiology, medicine, surgery, pathology, prosthesis, patient care, dentistry, athletics and even social and environmental studies The domain of the subject extends to rehabilitation of patients, mechanical analysis of clinical treatments and design of compatible prostheses and instruments for use by humans.
![]()
Vehicles that move in land and air have revolutionized transport. The number of vehicles is increasing rapidly but the total road length and road width are not increasing in the same proportion. The economic impact of vehicles is significant. It will be difficult to manage things without the use of efficient transport system. But there are also some problems which require enough attention: pollution and accidents. Everyday we read and hear news of traffic accidents. The loss of life and property is truly staggering. Many people of productive age group die and many others are physically disabled leaving a long term socio-economic effect.
Good engineering design of vehicles can reduce the severity of vehicle impact upon the passenger as well as the vehicle. Also, better design of highways, proper use of traffic rules and regulations and awareness among people are helpful in prevention of accidents. The overall solution of vehicle impact problem involves aspects ranging from design to behavioral sciences. Of course there is no panacea that immediately solves the problem of survival after vehicle impact.
During an impact, the tissues of body are subjected to different types of stresses. Rupture and distortion of the tissues involve series of biomechanical processes. The damage that occurs to the brain-box (cranium) causes the largest number of fatalities. Results from biomechanical analysis of impact problem are useful in clinical treatment, rehabilitation, impact-prevention, severity-minimization and designs.
Statistical profile shows that number of accidents (of all types) is decreasing every year but the motor vehicle accidents are increasing. At present, in most developed countries and developing countries, about half of all accidental deaths are attributed to vehicle related causes. Two of the important resources that a nation has are its people and the time they can constructively devote to the development of the nation. The mean age of fatality victims is about 30 years. If we suppose the average life expectancy in developing countries to be 60 years, the number of man-years lost due to a single fatality is 30. Besides, the pain and suffering of the victims and their families cannot be quantified but are as important, if not much more so, than economic aspects.
Mechanical analysis of impact problem:
The kinetic energy of a moving vehicle is half the product of its mass and the square of its velocity. Hence kinetic energy has exponential relation with velocity. A small vehicle moving with greater velocity will have greater kinetic energy than a larger vehicle moving with smaller velocity. Larger amount of energy means a large impact during the accident. Energy dissipation is an important part of vehicle –accident. When the energy involved is greater the occupants of the vehicle have to bear more stress. Greater magnitude stresses cause fractures and dislocations of tissues. Cranium gets damaged by excessive stress on the flat bones. Researches conducted in the field show that fatality rate increases with the velocity of the vehicle at the impact time.
Whenever an accident occurs, a series of collisions follows. First the vehicle collides with an external body or a moving vehicle suddenly comes to rest. Next the occupant of the vehicle collides with the interior of the vehicle and this is often called second collision. Other collisions can follow inside and outside the vehicle.
In vehicle accidents, parts in the interior of the vehicle cause different types of injuries to the occupants. In most cases steering assembly causes major injury. Next, the instrument panel causes large number of injuries. Windshield and door are other parts causing significant number of injuries. During the accident, injuries are likely to occur in different parts of the body. On this basis there are grater chances of head injury first and this injury is more severe than the injuries in legs, arms, chest and the abdomen. Head injury is the cause of fatality in ¾ of all cases. Next leading cause is chest injury.
It is difficult to quantify the injury criteria in a meaningful manner. Head injury is the main cause of fatality. The severity of injuries due to internal collision can be minimized by designing a safe interior in the vehicle but most of the time manufacturers are busy improving the exterior looks and attractiveness of the vehicle body.
Data on human volunteers and animals have been accumulated by different institutions working in the field of impact biomechanics. Analysis of the data shows following results.
A vehicle suffering a major collision is subjected to a large deceleration at the beginning and the deceleration slowly drops till the velocity reaches zero.
Let the deceleration be denoted by ‘a’: a is a variable with respect to time.
The average deceleration at any instant is inversely proportional to the time elapsed after the collision.
![]()
The graph of deceleration Vs time is a perfect hyperbola suggesting the following mathematical equation.
![]()
The curve obtained is tolerance curve. The impulse level tolerable by the brain before undergoing permanent damage or skull fracture cannot be however determined so easily. Equation (1) can be plotted on a log-log basis.
Accordingly :
![]()
In the form of y + x = constant.
The slope suggested by the equation is -1 but the actual experimental data indicate a slope of -1/2.5.
This suggests a new form of log equation.
![]()
Where n = 2.5
So,
![]()
Hence,
![]()
The deceleration is expressed in terms of ‘g’ (acceleration due to gravity), the severity index can be scaled in such a way that a value of approximately 1000 units is the borderline between fatal and nonfatal impacts. This criterion is Gadd criterion of impact evaluation.
Strength of tissues:
The force bearing elements in tissues are mainly collagen, elastin, fluids and bones. Human body is not a homogeneous system. Different constituent tissues of body parts have different force bearing capacities.
The Young’s modulus for elasticity of collagen is about 4.4 x 108 N/m2 . Same for elastin is 3.8 x 105 N/m2.
Collagen is more elastic than elastin in the language of mechanics. But collagen is less extensible than elastin. Maximum strain tolerable by collagen fibers is about 10% where as elastin is capable of extension up to 100% additional length. Hence ligaments made of elastin are more susceptible to damage than tendons made of collagen.
In bone there are two main force-bearing-constituents namely apatite and collagen. The strength of bone depends upon proportion of various stress bearing elements present in it.
Table 1: Strengths of some selected bones
|
SN |
Bone Type |
Tensile strength |
Compressive strengths |
|
1 |
Humerus (Hand) Long |
10.71x 107 N/m2. |
12.8x 107 N/m2. |
|
2 |
Femur (Leg) Long |
8.5 x 107 N/m2 |
18.57 x 107 N/m2 |
|
3 |
Fibula (leg) Long |
8.3 x 107 N/m2 |
17.8 x 107 N/m2 |
|
4 |
Parietal (Cranium) flat |
7.14 x 107 N/m2 |
15.7 x 107 N/m2 |
If P is the total load borne by the bone:
Load borne by apatite
Load borne by collagen
Here:
Aa: cross sectional area of apatite, Ac: Cross section area of collagen
Ea: Modulus of elasticity of apatite, Ec: Modulus of elasticity of collagen
P : Load borne by whole bone Wa: Load borne by apatite
Wc: Load borne by collagen
During accidents body parts are acted upon by a sudden impact load and the energy imparted upon them by the impact is huge. The strength of the tissues now depends upon the maximum impact energy which they can absorb. According to this, soft tissues like muscles, blood vessels, tendons and ligaments are more prone to permanent damage. Also the brain box cannot dissipate high impact energy.
Maximum stress intensity due to a suddenly applied load is twice the stress intensity produced by the load of same magnitude applied gradually. This can be easily derived from basic equations of solid mechanics.
Maximum stress due to a load applied suddenly = 2 x stress produced by same load applied gradually.
In this way, a force that the cranium can tolerate in normal condition may break it open during impact load condition. In other words the stress bearing capacity during impact is substantially reduced.
General Injury Analysis:
a) Brain Damage: /Head injury
Scalp damage: includes bruises, abrasion, laceration of skin.
Skull fracture may be of four main types:
i. Depressed Fracture
ii. Linear or Stellar Fracture
iii. Indented Fracture
iv. Crushed Fracture
Brain damage involves impairment of neural function due to mechanical force. Also internal bleeding in brain may cause functional impairment. Most serious form of brain damage occurs when the brain tissues undergo laceration or tearing. Symptoms of brain damage manifested by vehicle impact victim are:
i. Loss of coordinated response to external stimuli
ii. Respiratory pause (apnea) by 20 to 30 beats/ minute (Bradycardia)
iii. Loss of corneal and palpebral reflexes.
iv. Loss of voluntary movements.
Cause: Brain damage can be produced either by a blow or by acceleration of the head without collision; cranium is like a fluid filled cavity. It contains nervous tissue surrounded by CSF (Cerebro Spinal Fluid).
b) Tissue rupture/ Bone fracture/ dislocation:
A static or impact force can produce tensile stress/compressive stresses or shear stress on the tissue depending upon the direction of its application. Tensile and compressive stresses may bring ruptures and fractures in the tissues while the shear stress generally dislocates the tissues from their normal position (as in knee, ankle dislocation).
Impact Effect Minimization and Impact Prevention:
Much of the attention has been given to frontal-impact-response study in case of brain damage. To understand the entire biomechanical effects non frontal impact study should be given equal importance.
As a protective measure the vehicles can be fitted with air bags controlled by deceleration transducers. The bags are inflated upon sudden deceleration and gas under high pressure is utilized for that. The passenger presses against the air bag and slowly comes to rest during which the bag gets deflated. Air bag system is not equally suitable for people of different age groups. Also the high noise level associated with inflation of the bag can affect the ears of the passengers.
Seat belts are also useful means to prevent second collision. The interior of the vehicle should not have lacerative potential. This should be taken into consideration while furnishing the inner part of the vehicle. The automobile industries have been exerting most of their energies toward insulating the occupants from vertical motions to make the ride increasingly smooth. No attention has been given to prevent the horizontal motions that occur during impacts. Most of the injuries producing accidents are due to human error than vehicle failure. The obvious need is energy absorbing system. In vehicle industries the word ‘crashworthiness’ denotes good energy absorbing capabilities during an impact situation. We can differentiate external crashworthiness from internal crashworthiness. During an impact the front and sides of a vehicle get deformed by absorbing energy. During the second collision the occupant strikes a portion of the interior, which is well designed, absorbs a significant amount of occupant kinetic energy. The environment immediately enclosing the occupant, with which he may make contact during second collision is here referred to as internally energy absorbing or alternatively, internally crashworthy. Air bag falls into the category of internally energy absorbing device. Airbags should be fitted in front and rear seats taking enough consideration of strengths of seats. Also it is safe to provide air bags on the sides of the occupant to prevent collision with door.
To make the vehicle externally crashworthy vehicle body should be made of proper metals and materials. The materials used in vehicle exterior should be tested for their strength and impact coefficients. Metals capable of absorbing large amount of impact energy should be used in the vehicle architecture. The crashworthiness design is equally important for aircrafts. In aircrafts it has been seen that the external crashworthiness is appreciable but when it comes to the question of internal crashworthiness most of the fatalities are due to absence of proper energy absorbing system in the interior.
Summary: Every year a number of people die and many others are permanently disabled, in economically productive age, due to vehicle accidents. The loss caused to the nation is great and he sorrow and pain of the concerned families are immeasurable. Different body parts respond differently to impact loads. Biomechanical analysis of the problem provides information useful in the clinical treatment of the victims and the inferences reached are equally useful in design of crashworthy vehicles. Special attention should be given to insulate brain box from large impact conditions for brain damage is main cause of fatality in vehicle accidents. Safety measures should be taken by all concerned parties to prevent and minimize the effects of vehicle impact.
References:
JSME (Japanese Society of Mechanical Engineers) International Journal
Special Bioengineering Issue March 1999
Jurd, Richard D : Instant Notes on Animal Biology
Viva Books Pvt Ltd New Delhi 1998
Kummer, Benno ‘Biomechanics of Bone’: Fung Y.C. et al ‘Biomechanics its foundation and objectives’ Prentice Hall USA 1978
Perrone Nicholas ‘Biomechanical Problems related to vehicle impact’: Fung Y.C. et al ‘Biomechanics its foundation and objectives’ Prentice Hall USA 1978
Ramamurtham S & Narayan N ‘Strength of Materials’ Dhanpat Rai New Delhi 1998
Werner G ‘Biomechanics of Head Injury’ Fung Y.C. et al ‘Biomechanics its foundation and objectives’ Prentice Hall USA 1978
Zweifach Benjamin ‘Biomechanics & Physiology’: Fung Y.C. et al ‘Biomechanics its foundation and objectives’ Prentice Hall USA 1978
FINGERPRINT AS A BIOMETRIC IDENTITY
Puskar Raj Chapagain
Department of Physics
With the increase of online communication and transactions, the demand for security and privacy has been increased. There are several solutions already in use to protect confidential information and to authenticate people electronically. When biometrics is used, it enhances the privacy and integrity more than that of other methods. The main objective of this article is to explain how fingerprint verification, personal tokens and Match-On-Card technology can help ensure integrity.
Introduction:
Biometrics means recognizing an individual based on physical
or behavioral characteristics. The most common biometric is
fingerprint, but also in use are facial, iris, hand, and
voice technologies. With Match-on-Card, biometrics are used
to verify a persons identity based on an enrolled template,
stored on a smart card, compared against a live biometric
sample-most often a fingerprint.
When a fingerprint image is enrolled, only a part of the information is stored. This information extract is called a template. It is not possible to reconstruct a fingerprint image from a template; i.e the transformation process is non-reversible. There are two ways to store fingerprint templates; database storage or storage in a personal token. A database with fingerprint templates of individual cannot be searched with a fingerprint template from a personal token, as the template is never allowed to leave the storage in the security context, such as a Smart Card. A Smart card is a plastic card, which holds a processing chip. The chip on the card is designed to protect the information stored on it using various security mechanisms.
Biometrics as Digital Identity:
Public Key Infrastructure, PKI, comprises all necessary functions to achieve non-repudiation, encryption, digital signing and strong authentication. Still, while PKI delivers the framework for all this functionality, the problem of verifying the users’ identity remains. The main methods of verification of PKI are:
· Any key, Smart Card or other tokens that individual use to verify one’s identity.
· A PIN or password that only the concern person knows.
The problem with these two methods is that they can be borrowed or stolen. Biometrics represents the third alternative:
- Individual’s fingerprint, iris, voice etc.
These three methods are often combined, where one part identifies the user, while the other verifies that the person who he/she claims to be. e.g. a Smart Card (something individual has) in combination with fingerprint verification (something individual is).
Using digital certificates protected with biometrics is the best way of proving a person's identity. The biometric method most commonly used is fingerprint verification. Fingerprint verification is seen as the best solution with regards to convenience, cost efficiency and reliability.
Use of Fingerprints and Personal Tokens:
a. Database storage – Identification:
Databases with fingerprint templates are used by concerned authorities. The idea is to check fingerprint images from people against this database while investigating a case. This process is called identification; as we have found this fingerprint we will check the data base to see if we find a match among our registered persons. The idea of having fingerprints collected and templates stored in a database together with information about the user is not appealing to many people. Some claim these databases are a threat to privacy.
b. Personal token–Verification:
When talking about tokens, we often refer to Smart Cards. Smart Cards are widely used for everything from bus tickets to carrier of digital certificates, which are used to access various electronic services. The reason for using a Smart Card is that it is tamper resistant; it is very hard to hack a Smart Card. This also makes the Smart Card a suitable carrier of biometric templates. In this case the Smart Card is used for identification, and the user verifies the ownership of it. For example, for digital signing of a contract, the user presents the Smart card to the card reader and then puts his or her finger on the fingerprint sensor. If the presented fingerprint image matches with the template stored in the Smart Card, the contract is signed with the user’s cryptographic key stored in the card (Figure1). With the Match-On-Card technology the fingerprint is verified inside the secure environment of the Smart Card. In this case the fingerprint template stored on the Smart Card cannot be extracted. It can only be used internally by the Smart Card itself. Signing contracts or documents is only one application where the biometric verification in Smart Cards can be used. Other applications might be ID cards, where the user proves the validity and ownership of the ID card by biometric verification.
Match-On-Card has been included in many standards around the world. The international standards body- ISO is completing several standards for biometrics. New rounds of those standards promise to include Match-On-Card.
Figure 1: The figure shows an example of the usage of fingerprints for verification. The fingerprint is used to verify the ownership of the smart card, to be able to use the cryptographic keys for digital signatures and encryption.
c. Using Smart Cards and Fingerprint Verification:
Fingerprint verification is considered the most viable technology when biometrics is to be used with maintained integrity (Table1). The only commercially proven biometric technologies suitable for Smart Cards, using Match-On-Card technology, are fingerprint and voice verification, where finger-prints have far better performance with regards to accuracy. The usage of Smart Cards and Match-On-Card technology is very important for protecting biometric templates against tampering.
Table 1: Ranking Different Biometrics
|
Rank |
Accuracy |
Convenience |
Cost |
Match-On-Card |
|
1 |
DNA |
Voice |
Voice |
Finger |
|
2 |
Iris |
Face |
Signature |
Voice |
|
3 |
Retina |
Signature |
Finger |
|
|
4 |
Finger |
Finger |
Face |
|
|
5 |
Face |
Iris |
Iris |
|
|
6 |
Signature |
Retina |
Retina |
|
|
7 |
Voice |
DNA |
DNA |
|
(Source: Morgan Keegan & Co report)

Conclusion:
When using biometrics in combination with a personal token, e.g. a Smart Card - no database of fingerprint templates is needed. No one has access to the stored fingerprint template, not even the owner, since the template cannot be extracted from the card. It can only be used internally in the card where it is used for matching against the fingerprint of the person who claims to be the owner of the card. It is in this case not possible to misuse the fingerprint template, nor the users’ identity.
References:
1. www.siemens.com
2. www.morgankeegan.com
3. www.rsa.com
4. www.infineon.com
TISSUE ENGINEERING: A MULTIDISCIPLINARY FIELD OF BIOMEDICAL ENGINEERING
Tissue engineering is the field of biomedical engineering that unites biology, engineering and medicine to restore or replace tissues or organs damaged by disease, injury or congenital anomaly[1]. In vitro tissue engineering deals with the reconstruction of tissues or organs outside the body. The reconstructed tissues or organs will be reimplanted for the proper cure of the disease or defect. In vivo tissue engineering deals with the modifications of the existing tissues inside the body by promoting their growth and repair[2].
General Principle

Basic Principle of Tissue Engineering
The required cells are extracted and are preserved using different chemicals[4]. The extracted cells/tissues are isolated and are differentiated. These are the initial materials required for tissue engineering. Then, seeding of appropriate cells is performed in a scaffold (natural or synthetic) configured in an appropriate shape, after which growth factors are added. The phenomenon is then followed by different external guides and signals such as mechanical stresses and strains that are applied to make cells grow into functional 3-D structures.
Major Equipment Involved in Tissue Engineering
There are different equipments involved in Tissue Engineering such as Laminar Flows, Incubators, and Bioreactors etc. One of the major is bioreactor.
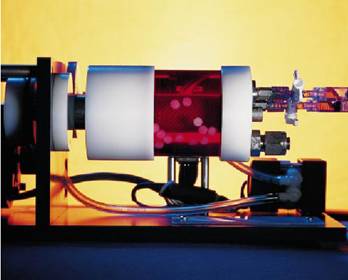
Bioreactors
A bioreactor is a device or a system meant for the growth of cells and tissue (in the context of Tissue Engineering) and their preservation that supports a biologically active environment. It is a vessel in which a chemical process is carried out involving organisms or biochemically active substances derived from such organisms. They are commonly cylindrical in shape, often ranging from some litres to cubic meters, and are often made of stainless steel.
Bioreactors are required to orient and configure three-dimensional shapes to the tissues and organs like heart, kidneys, pancreas etc under controlled pressure, temperature, pH and agitation speed or rotation to perform their desired function with great efficiency. Bioreactors are aimed to provide native environment to the developing organs as is provided within the biological body.
Bioreactor
Bioreactors are controlled by PLCs (Programmable Logic Controllers), which are computer-based systems used for the automation of real world processes, such as control of machinery like bioreactors aimed to grow bioartificial organs. The input/output arrangements connect PLC to the sensors and actuators. PLCs read the complex position system of the equipment and sometimes machinery vision as well. These devices are programmed by using structured programming languages like ‘C’ and logic elementary operations[5].
Present Commercial Applications of Tissue Engineering in Human System
There are many commercial applications of tissue engineering at present, out of which some of the major applications are as follows.
Cartilage repair
Cartilage is a vascular in nature. Thus, healing of any wound in it, especially in articular cartilage, is really tedious. Tissue Engineering has become a tool for regeneration of articular cartilage.
Chondrocytes are extracted from the part of cartilage that is not defective; after which, cells are seeded in a biodegradable, hybrid scaffold of Poly Lacticglycolic Acid (PLGA) and collagen. Seeding efficiency is raised by hybridization. PLGA provides appropriate mechanical strength to the cells and collagen facilitates homogenous cell distribution. The rate at which matrix (scaffold) degradation occurs has to be coincided with the tissue formation so that, while the cells are fabricating their own natural matrix structure around themselves, the scaffold is able to provide structural integrity within the body and eventually it will breakdown leaving the neotissue, which will take over the mechanical load. Hence, the defected cartilage is repaired[6].
fig. fig. cartilage repair
Vessels Repair
When blood vessels are damaged or blocked or dilated (aneurysm), then autologous veins are used to replace the damaged part, but this is not always possible. The other alternatives are artificial grafts or construction of bioartificial vascular grafts, which can be later implanted into the body[7].


Vessel Grafts Cartilage Repair
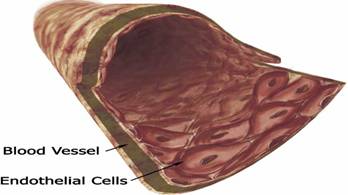
A collagen based matrix is contracted into a tubular biopolymer scaffold by smooth muscle cells and is seeded by endothelial cells. The isolation, purification and seeding of endothelial cells is automated. To reduce the immunogenecity, endothelial cells are recruited from the patient himself/herself. Research conducted in Georgia Technology Emory Center has found that mechanics can influence the function of the bioartificial tissues. Application of cyclic strain force to Neremy bioartificial blood vessels model during tissue engineering in the lab has improved its mechanical strength and structural organization.
Nerves Regeneration
Deficiency of some specific neuro-active substances (neurotransmitters) results in neurological disorders. Tissue engineered composites like nerve growth factors can be designed in such a way that they can cross the blood brain barrier and thus have the potentiality to rectify defects associated with the brain tissues such as thosefound in Alzheimer’s and Parkinson’s diseases.
Polymeric tubes are implanted in the damaged parts of nerves and the nerves are grown in the designated direction. Growth and development of nerves occurs due to angiogenesis[8].
Bone Reconstruction
Bone ordinarily heals itself if fractured, but if a section is lost through disease or an accident, that section will not be generated in an adult human. The use of tissue engineered bone may be an effective approach to the treatment of bone loss due to trauma or disease.
When coral (porous hydroxyapatite) is seeded with bone marrow cells, or with the cells derived from periosteum and is placed in subcutaneous tissue that is not adjacent to the native bone, new bone forms. After performing scaffolding-guided tissue engineering, it is later implanted into the targeted area (i.e. defected bone), which results in the recovery of the defective part and functional restoration of a stable and biomechanically sound bone of normal length and strength takes place[9].
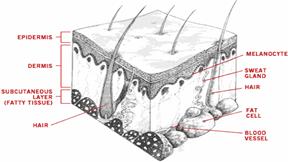
Regeneration of Skin
Thousands of people around the globe are dying of burn wounds and diabetic ulcer and thousands of people undergo different therapies from grafting cadaver skin to using artificial skin to promote healing wounds as early as possible. Therefore, the concept of tissue engineering in skin regeneration has been launched. These products are revolutionary because they allow the actual regeneration of skin badly damaged by burns or other traumas, ulcers and tumors rather than the formation of scar tissue.
The human infantile foreskins harvested by circumcision is the main source of living human skin that is engineered in the laboratory, and is then used to patch the sites of fresh wounds. Appropriate medium containing nutrients and growth factors is provided during tissue culture, which when engineered increases in number. After developing engineered skin tissues, they are implanted into the fresh wounded part as a permanent cure. Thus, skin regeneration has promoted skin replacement therapy to the maximum that is highly applied to treat diabetic foot ulcers, burn wounds and venous ulcers as well[11].
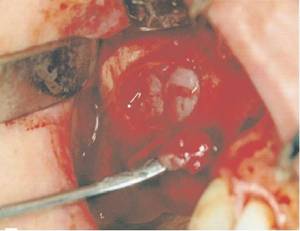
Development of Heart Valves
Defective heart valves make a considerable number of peoples’ lives miserable and they are subjected to death due to the lack of cure. Artificial heart valves are used for therapeutic purposes, but it is very expensive and at the same time the patient needs to take anticoagulant drugs throughout his/her life, which is not always possible. To overcome this problem, tissue engineering approach has been adopted to develop heart valves. A Typical Skin
A porcine heart valve is extracted (i.e. from pigs) and is then engineered using a scaffold where the heart valve is sutured and is preserved to suit human heart under lab conditions using different chemicals and biological environment. Finally, the heart valve along with the scaffold is implanted within the patient’s body to replace the existing defected heart valve.

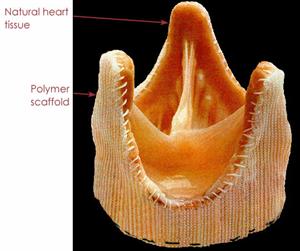
A Typical Human Heart Valve A Typical Porcine Heart Valve
Prospects of Tissue Engineering
Various researches are being carried on to develop new organs in the laboratory. Although production of bioartificial organs like heart, kidneys, liver, pancreas etc through tissue engineering is not yet successful, NASA's Tissue Bioreactor has succesfully grown heart tissue, skeletal tissue, ligaments, cancer tissues for study and researchers are trying to vascularize such vital organs, which is a major hurdle[12]. Scientists are trying to develop chondrocytes from undifferentiated cells called fibroblasts, which if succeeded, will help solve the problem of chondro-osteoarthritis[13].
In Nepal, College of Biomedical Engineering and Applied Sciences (CBEAS) has been established realizing the need and importance of research-based engineering approaches. The roadmap of Bone Banking has been prepared that involves the concept of tissue engineering for the preservation of bones. Tissue engineered heart valves and regenerated skins might be available very soon within the country to replace defected heart valves and to operate skin replacement therapy respectively.
Conclusion
Despite ethical challenges, tissue engineering is gaining its momentum to substitute other complicated and expensive surgical procedures like organ transplantation and grafts. Thus, living cells seeded with synthetic scaffolds give rise to the regeneration of new tissues, the process known as tissue engineering[14], a multidisciplinary field of Biomedical Engineering, which is a boon to the arena of Medical Science with the application of engineering technology.
References
[1] PTEI(Pittsburg tissue engineering initiative) accessed on 15th Dec. 2005
[2] Biomaterials(Tissue engineering) ;Francois Berthiaume , Mehmet Toner, Ronald G. Tompkins and Martin L. Yarmush
[3] Wikipedia.org, an on line encyclopaedia accessed on 21st Dec. 2005
[4] Biomaterials(tissue engineering) ; Francois Berthiaume , mehmet Toner, Ronald G. Tompkins and Martin L. Yarmush
[5] Wikipedia, an on line encyclopaedia accessed on 14th Dec. 2005
[6] www.ncbi.nlm.gov/entrez/query.fegi accessed on 16th Dec. 2005
[7] www.liv.ac.uk accessed on 14th Dec. 2005
[8] Biomaterials (Tissue Engineering);Francois Berthiaume , Mehmet Toner, Ronald G. Tompkins and Martin L. Yarmush
[9] www.nejm.org accessed on 16th Dec. 2005
[10] (New England Journal of Medicine, 2001 344:1511) by C.A. Vacanti
[11] Engineering Human Tissue by Steve Alan Edwards
[12] Wikipedia, an online encyclopaedia accessed on 20th Dec. 2005